Mi Hao, Yan Cheng, Jie Wu, Yu Cheng, Jing Wang
Department of Ophthalmology, First Affiliated Hospital of Northwest University, Xi’an No.1 Hospital, Shaanxi Institute of Ophthalmology, Xi’an 710002, Shaanxi Province, China
Abstract
● KEYWORDS: recombinant human nerve growth factor;neurotrophic keratitis; corneal subbasal nerve
Neurotrophic keratitis (NK) is a degenerative disease of the cornea caused by trigeminal nerve injury, including virus infection, trauma, surgery, inflammation and other factors, decreased corneal perception and nutritional disorder after denervation, weakened defenses against external harmful factors, dry eye, corneal epithelial defects and corneal ulcers,and corneal stroma melting and perforations[1].
The principle of NK treatment is to prevent the progression of corneal injury and improve corneal trigeminal innervation,to restore the nutritional supply of corneal nerves, and promote corneal renewal and healing[2]. Current treatments for NK include autologous serum, preservative‐free artificial tears, a corneal bandage lens, and an amniotic membrane transplantation[3]. The best treatment involves restoring the trophic supply of corneal nerves, as well as stimulating corneal re‐innervation and healing. As a neurotrophic factor and immunomodulatory factor, nerve growth factor (NGF) plays an important role in the survival, growth, and differentiation of sensory neurons, as well as in promoting wound healing[4].Recombinant human NGF (rhNGF) has the same structure as endogenous NGF, so it can quickly promote corneal wound healing and improve the corneal perception and tear production[5].
RhNGF (cenegermin, 20 μg/mL of rhNGF) has been clinically used in Europe, United States,etc, and has been shown to aid in the recovery of corneal nerve function[6‐8]. Cenegermin has been presently approved for clinical treatment of moderate or severe NK, which is the only effective biotherapy for clinical treatment of this disorder, but there is no relevant research reports in China. The purpose of this study was explored the clinical efficacy of rhNGF for corneal nerve regeneration and corneal epithelial healing in NK patients in China.
Ethical Approval This study was approved by the Ethics Committee of Xi’an No.1 Hospital (Approval No.2021‐11),and followed the tenets of the Declaration of Helsinki. The number of Clinical Trial Registry is ChiCTR2100053592. The diagnosis and treatment processes were described in detail to the patients and their families, and informed consent was signed with the consent of the patients’ families.
Six patients (nine eyes) with NK diagnosed in our hospital from January 2021 to June 2021 were collected. All patients received cenegermin six times a day for 8wk. Other drugs included 0.05% cyclosporine eye drops, twice a day; 0.3%gatifloxacin eye drops, twice a day; and vitamin A palmitate ophthalmic gel once a night. At baseline and at 2, 4, 6, and 8wk of treatment, the patients underwent eye examinations,including visual acuity, slit lamp examination, corneal fluorescein staining,in vivoconfocal microscopyetc.
Inclusion criteria included patients diagnosed as moderate or severe NK at our hospital. And after more than 4wk of traditional treatment, including antibiotics, artificial tears,autologous sera, corneal bandage lensesetc, the corneal lesion area still was not healed, the depth of keratopathy was less than two‐thirds, and there was no perforation and/or stromal melting.
Exclusion criteria included infectious corneal ulcers,peripheral corneal ulcers associated with autoimmune diseases,endophthalmitis, corneal dystrophies, glaucoma patients who needed to change the treatment plan midway according to the specific conditions of their eyes, and patients with loss of follow‐up and incomplete data records.
在实践活动中,学生可以充分了解我国目前食品安全现状和食品质量安全管理的具体措施和发展进展,增强学生对于该课程的兴趣和学习的动力,加深作为一名食品质量安全管理专业大学生的责任感,以及学习该课程的重要意义所在。
Visual acuity examination was conducted using the international standard visual acuity chart, and the best‐corrected visual acuity(BCVA) at baseline and 8wk after treatment were recorded.
For the corneal fluorescence staining score, sodium fluorescein was dropped into the conjunctival sac of the affected eye, the staining of the corneal epithelium was observed with cobalt blue light under a slit lamp, and the corneal staining results were recorded using a 0‐12 point scale. First, the cornea was divided into four quadrants involving the supranasal, infranasal,supratemporal, and infratemporal quadrants. According to the degree of staining and staining area, it was divided into 0‐3 scores (0: no staining, 1 scores: less than 5 points, 3 scores:flake staining, and 2 scores: between 1 and 3 scores).
For in vivoconfocal microscopy (IVCM; HRT II Rostock Cornea Module; Heidelberg Engineering, Heidelberg,Germany), the central part of the cornea and the superior,inferior, nasal, and temporal quadrants were scanned, and the NeuronJ analysis plug‐in in Image J software (National Institutes of Health, Bethesda, MD, USA) was used to track the density and the number of nerve branches of the corneal subbasal nerves. The images were processed anonymously before analysis to avoid statistician bias. The nerve fiber density was calculated in μm/mm2. In each picture, the number of subbasal nerve fiber branches and nerve fiber bifurcation points were counted and reported as numbers. Ten different IVCM images were selected to calculate the average corneal nerve density and number of nerve branches and bifurcations.For the corneal sensation test, cotton was twisted at the end of the disinfection cotton swab into a slender cotton yarn and bent to 45° with the cotton stick. The approach involved the side of the tested eye with the tip of cotton filament, which gently touched the cornea. The resulting judgments involved those with normal corneal sensation who immediately had a reflex blink or perception response. The absence of a blinking reflex indicated a decrease or disappearance of corneal perception.The tear index used the Keratograph 5M (Oculus, Wetzlar,Germany), which automatically measured the height of the tear river before and after stimulation during non‐contact conditions. A LipiView II interferometer (TearScience Inc,Morrisville, NC, USA) used the white light interference principle and specular reflection method to directly evaluate the color of the tear film interference light, indirect measurement of lipid layer thickness (LLT).
For the conjunctival impression cytology (CIC) examination,a prepared cellulose acetate filter paper was taken from the conjunctiva of the lower eyelid after ocular surface anesthesia and placed on a slide. A total of 1‐2 drops of 100 mg/L acridine orange saline solution was added to the filter membrane. After 3‐5min, the fluorescence was observed using a fluorescence microscope. According to the number and morphology of cells attached to the filter paper, the cells were graded according to the Tseng classification[9](grade V).
For the tear ferning (TF) test, tears from the fornix of the affected eye were collected with a capillary glass tube and coated on clean slides. After drying, according to the appearance of the crystal‐like branched ferns, it was roughly divided into four grades: grade I was a large and compact continuous dendritic distribution; grade II was a small, sparse, and scattered dendritic distribution; grade III was rarely a dendritic distribution, accompanied by a large number of vacuoles; and grade IV was a complete loss of fern‐like appearance, with only the clustered mucus.
Statistical AnalysisThe data were analyzed by SPSS statistical software for Windows, version 23.0 (SPSS, Chicago,IL, USA). The Shapiro‐Wilke test was used to test the normal distribution, and the mean and standard deviation (SD) were used to represent mean±SD. Variables in accordance with the normal distribution were analyzed by repeated measurement analysis of variance, and variables that did not correspond with the normal distribution were tested using a nonparametric Friedman test. All tests were two‐sided and a level of statistical significance was set atP<0.05.
The general data of six NK patients in this study are shownin Table 1. All patients were from 4‐61 years of age, with an average age of 32.17±22.55y. There were four females and two males, as shown in Table 1.
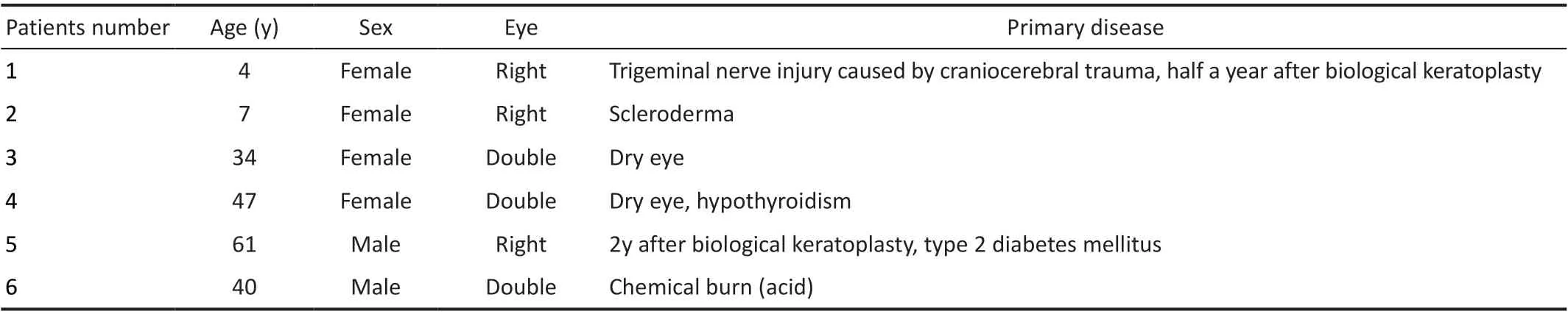
Table 1 General data of patients

Table 2 Changes of corneal fluorescence staining score, conjunctival imprinting cytology, and the tear fern test at baseline and after rhNGF treatment mean±SD
The average BCVA of NK patients at baseline and 8wk after treatment were 0.27±0.51 and 0.18±0.33, respectively(P=0.414). It could not be determined whether the visual acuity of patients with NK could be improved after treatment.Corneal fluorescence staining using a slit lamp showed that all patients had corneal epithelial defects. After 2wk of treatment, complete corneal healing was observed in two eyes of one patient; after 4wk of treatment, corneal ulcers were completely healed in four eyes of three patients; and after 8wk of treatment, all corneal ulcers of patients were completely healed. After 8wk of rhNGF treatment, the score of corneal fluorescent staining was significantly lower than that of the baseline, and the difference was statistically significant(P<0.01), as shown in Table 2.

Figure 1 Changes of the corneal nerve fiber density at baseline and after rhNGF treatment.
Regarding morphological changes of corneal nerve fibersin vivousing confocal microscopy, at baseline, the corneal subbasal nerve fibers of NK patients were sparse, uneven in thickness, and irregular in course. After 8wk of treatment,the density of corneal subbasal nerve fibers increased and progressed normally. Table 4 shows that the density of subbasal nerve fibers significantly increased from the second week to the eighth week after treatment, which was statistically significant (P<0.01). At the same time, Figure 1 shows that the corneal nerve fiber density increased gradually with the progression of treatment. When the density of nerve fibers increased, the number of ramification and bifurcation points of subbasal nerve fibers significantly increased (P=0.001,P=0.003).Figure 2 shows that an NK patient’s IVCM images.Regarding corneal sensation, because of the limitation of conditions, the corneal sensation of patients could not be measured quantitatively in the course of this treatment.We only measured the changes of corneal sensation using the cotton silk method. At baseline, the corneal sensation decreased in eight eyes and disappeared in one eye, and after 8wk of treatment, the corneal sensation was basically normal in two eyes, decreased in six eyes, and disappeared in one eye.

Figure 2 In vivo confocal microscopy analysis Representative images of a case of NK, male, 40-year-old, affected by chemical burn (acid). A:The nerve fibers evaluated at baseline were sparse, uneven in thickness; B: Nerve fiber density, ramification and bifurcation point showed a significant increase at week 4 of treatment with recombinant human nerve growth factor; C: The improvement was maintained at the 8-week follow-up.

Table 3 Changes of the tear indices in patients at baseline and after rhNGF treatment mean±SD

Table 4 Changes in the density, branching, and bifurcation points of corneal nerve fibers at baseline and after rhNGF treatment mean±SD
The cornea is innervated by ocular branches of the trigeminal nerve, including the long ciliary, short ciliary, and autonomic nerves. It is the most densely distributed tissue of nerve fibers in the entire body. The corneal nerve is very important in maintaining the stability of the ocular surface and the normal function of the cornea. It can trigger protective reflexes such as blinking and tears by causing ocular symptoms such as pain and irritation. It can also provide nutritional support for ocular surface tissue by releasing neurotransmitters, which promote wound healing and maintain the integrity of the anatomical structure. Corneal denervation causes decreased vitality, decreased metabolism, and mitosis of epithelial cells,with subsequent epithelial cell changes, including intracellular edema, loss of microvilli, and abnormal development of the basal lamina, accompanied by slow corneal wound healing[1,10‐11]. Sensory innervation injury leads to the decrease or complete loss of corneal sensitivity, resulting in refractory corneal ulcers, including NK.
Regarding the relationship between corneal nerve and epithelial cell integrity[12], the corneal nerve promotes corneal epithelial cell proliferation, migration, and differentiation, as well as nerve development and survival by releasing a variety of nerve mediators, which involve substance P, calcitonin gene‐related peptide, acetylcholine, norepinephrineetc. In addition, corneal epithelial cells release a variety of neurotrophic growth factors,including NGF, ciliary neurotrophic factor, and glial cell line‐derived neurotrophic factor, which are the basis of ocular surface balance and wound healing[13]. NGF can be synthesized and secreted by the corneal epithelium, stroma, endothelial cells, limbal stem cells, and conjunctiva. NGF can bind to two receptor proteins, high affinity receptor (tropomyosin receptor kinase A, TrkA) and low affinity receptor (p75 neurotrophin receptor, p75NTR), to maintain cell survival and promote cell migration, proliferation, and differentiation[14].
Boniniet al[15]reported that after treatment with 20 μg/mL rhNGF,the area of keratopathy was reduced by 49.8%, and corneal healing was 58.0% at week 4 (<0.5 mm lesion staining).At 8wk, 74.0% of the patients’ corneas healed. There was a significant difference between the 20 μg/mL rhNGF group and the control group (P<0.01). In the follow‐up of patients with corneal healing, there were few corneal epithelial defects or corneal ulcer recurrences. Pflugfelderet al[8]showed in a multicenter, randomized, double‐blind, case‐control study that corneal healing occurred in 16 (69.6%) of 23 patients treated with rhNGF at week 8, and seven (29.2%) of 24 patients in the control group (P=0.006). Our results showed that corneal healing was 44.4% at week 4 and 100% at week 8. Previous studies have also shown that corneal defects in the initial treatment were negatively correlated with the results the larger the defect, the less likely the healing[8,12].
Mastropasquaet al[7]evaluated the healing of the corneal nerve and epithelium after treatment of NK with rhNGF. The results showed that corneal ulcer healing was associated with corneal subbasal nerve regeneration, and the average density of subbasal nerve fibers was significantly higher than the baseline at the 4thand 8thweeks after treatment. The density of nerve fibers, the number of nerve branches, and the diameter of nerve fibers significantly increased, and the differences were statistically significant. These morphological changes were observed as early as 4wk after treatment, but the rate of improvement decreased after 4wk. However, the corneal nerve density, nerve fiber branches, and diameter did not reach values observed in the healthy control group. Our study showed that the density of subbasal nerve fibers and the number of nerves in NK patients significantly increased after treatment.The difference before and after treatment was statistically significant, but did not reach the corneal nerve fiber density of healthy patients reported in previous studies.
The complex relationship between corneal epithelial cells and nerves is very important in maintaining corneal physiological function and wound healing. The impairment of corneal perception will also hinder this nutritional relationship[12]. Previous studies reported that the corneal sensation was not completely related to changes of the subbasal plexus[16‐17]. It was therefore speculated that the sensory and nutritional functions of trigeminal nerve fibers existed as separate entities, at least partially independent of each other[18]. These results suggested that corneal perception measurement may not be sufficient to determine the specific nutritional functions of corneal nerve fibers. To characterize the structural changes of corneal nerve fibers, accurate imaging and quantitative analysis of the subbasal plexus are needed.IVCM is considered to be the gold standard for diagnosis[19].Previous studies[10]reported that the density of corneal subbasal nerve fibers in severe NK patients were lower than those in mild to moderate patients, which was similar to the decrease in corneal perception in mild to moderate patients, and was the most important diagnostic basis for the density and number of corneal nerve fibers. When the density of corneal subbasal nerve fibers significantly decreased in patients with mild NK,the risk of developing epithelial defects significantly increased.Persistent epithelial defects (PEDs) with severe reduction of the subbasal nerve are more likely to develop stromal ulcers,resulting in severe NK. Based on the results of the present study, we need to further quantitatively monitor corneal perception in order to determine changes in corneal nerve functions.
Deeks and Lamb[12]reported that the visual acuity of patients did not provide a statistically significant advantage after 8wk of rhNGF treatment, so the analysis of visual acuity may not necessarily reflect the severity or healing state of NK[15],when considering that the cornea is usually opaque during healing, and re‐epithelialization of the central or para‐central cornea may lead to optical aberrations, which leads to a loss of eyesight. The results of the present study showed that there was no statistical difference in visual acuity before and after treatment, which is consistent with previous studies. At the same time, it must be considered that it was related to scar formation in the process of corneal repair.Increasing evidence has shown that NGF regulated tear production and maintained tear film homeostasis, suggesting the potential role of NGF in the treatment of dry eye[20‐21], the increase of NGF in tears was the result of ocular surface injury in stimulating corneal healing. The researchers also studied the role of NGF in limbal stem cell differentiation, herpetic keratitis, dry eye, and corneal allograft rejection, suggesting that NGF was effective in the local treatment of other ocular surface diseases[22‐24]. NGF regulates tear film function through receptor‐binding nerve reflexes, which is expressed by tear glands, and induces goblet cell differentiation and mucin production[25‐26].Our results showed that the thickness of the lipid layer increased after 8wk of treatment with rhNGF. It was speculated that rhNGF promoted the secretion of lipid components by the Meibomian gland and maintained the stability of tear film by repairing corneal or conjunctival nerve fibers and improving the tear regulatory reflex pathway. The height of the tear river was no significant difference with baseline. According to the results of the CIC examination and TF test, the function of conjunctival goblet cells was not significantly improved.The possible reasons included the following: first, it has been thought that the height of tear river measured by an ocular surface analyzer and the height of tear river after stimulation may be affected by many factors; second, it may be related to the etiology of the patients, such as chemical burns and moderate and severe dry eye surface inflammation, resulting in conjunctival goblet cell damage; and finally, it may be related to the small sample size, which still needs to be increased in further studies.
In conclusion, we found that rhNGF can stimulate the healing of corneal epithelial cells, contribute to the repair and regeneration of injured nerves in Chinese patients with NK,and obtain a good clinical effect. However, this study failed to obtain the changes in the sensory function of corneal nerve fibers, which needs further study. In short, rhNGF is a welcome non‐surgical treatment option for this challenging degenerative disease.
Foundation:Supported by the Shaanxi Provincial Department of Science and Technology (No.2021SF‐331).
Conflicts of Interest: Hao M, None;Cheng Y,None;Wu J,None;Cheng Y, None;Wang J, None.
猜你喜欢 食品质量具体措施责任感 英国“大爷”的责任感华人时刊(2022年5期)2022-06-05提升食品质量与安全专业人才培养质量的探索食品安全导刊(2021年20期)2021-08-30标准化在食品质量安全保障中的重要性食品安全导刊(2021年20期)2021-08-30企业财务共享模式下防范财务风险的具体措施现代经济信息(2020年34期)2020-06-08国企如何实现“高质量”发展——要有“等不起”的紧迫感,“慢不得”的责任感当代陕西(2019年18期)2019-10-17加强施工质量监督的具体措施分析消费导刊(2018年10期)2018-08-20流行性腮腺炎(腮腺炎)的流行特征及预防控制疫情流行的具体措施分析中国医药指南(2017年3期)2017-11-13媒体品牌推广中的社会责任感新闻传播(2016年2期)2016-07-12加强大学生思想政治教育文化自觉性的意义和具体措施中国市场(2016年45期)2016-05-17食品质量安全的现状及对策现代食品(2016年14期)2016-04-28推荐访问:Human nerve recombinant